Hip Subluxation, Dislocation and Surveillance in Children with Cerebral Palsy (CP)
Children with cerebral palsy (CP) are at risk for hip subluxation and dislocation. Hip subluxation and dislocation occur when the hip joint is out of position. This happens slowly over time. The slow subluxation and dislocation in children with cerebral palsy is not the same as a sudden painful hip dislocation that can happen after an injury.
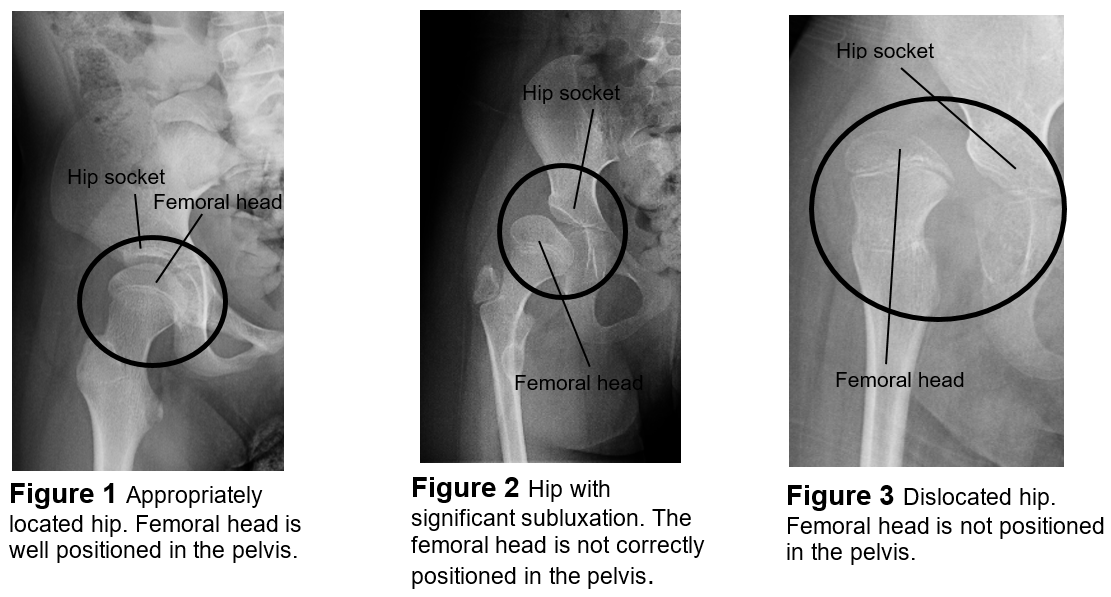
The hip is a ball and socket joint. The head of the femur (top of the thigh bone) is the ball and the part of the pelvis that meets the upper end of the thigh bone is the socket. When this joint works correctly, the ball moves freely in the socket and the leg moves without pain. When the ball is not fully in the socket it is called hip subluxation. Hip subluxation can cause limited range of motion of the hip and change growth of the femur and hip bone. Over time, a subluxed hip can become dislocated when the ball of the hip is not in the socket at all and can cause pain.
Hip dislocations can happen to only one hip, one hip and then the other hip, or both hips at the same time. Children with CP who can walk on their own or with little help are at lower risk for a hip dislocation than a child who cannot walk on their own.
How Hip Subluxation and Dislocation Happens
There is ongoing research to understand why hip subluxation and dislocation happens in people with CP. It is believed that there are many reasons.
- It may be caused by not putting weight on the legs. As a child grows and develops, the shape of the bones change through bearing weight (standing or walking). This helps keep the hip in its socket. If the child is not bearing weight, the hip cannot develop properly.
- Another reason may be related to muscle tone and spasticity (how muscles contract or stay tight). In many people with CP, the muscles that bring the legs together and into a sitting position are much tighter that the muscles that bring the legs apart and straight at the hips. This increased pull raises the risk for hip dislocations.
Pain With Hip Dislocation
Hip dislocations in patients with CP may be painful. For some, pain only occurs when their hip is moved to the side, such as for diapering or bathing. For others, the pain is constant no matter what the position. Dislocated hips that have not caused discomfort before can become painful.
Hip Surveillance
In children with CP it is important to monitor the hips with frequent x-rays and physical exams. This is called hip surveillance. This helps find problems so they can be treated early.
Hip surveillance cannot keep a hip from becoming subluxated and it cannot avoid the need for surgery. However, monitoring the hip can decrease the chance for hip dislocation by helping the care team make a plan to best help your child.
Every child with cerebral palsy needs at least one x-ray of their hips. This is normally done at the age of 2 years or soon after diagnosis with CP. More x-rays of the hips will be done depending on the child’s age, function level and if there is any concern for hip subluxation or dislocation during the exam.
Providers follow a standard care plan based on your child’s risk for dislocation to decide when they need x-rays. For example, children who walk usually have few x-rays. This is because of their decreased chance of hip subluxation and dislocation. Children who have trouble walking often have a higher rate of hip subluxation and have one x-ray, or more, each year. Certain results on a physical exam or x-ray may require your child to get- x-rays more often.
X-Rays for a Dislocated Hip
The only way to know if a hip is dislocated is to get an x-ray. However, there are some signs and symptoms that may give a clue that the hip is coming out of the socket:
- discomfort when moving the hip
- one leg likes to cross over the other and not move apart easily
- one leg appears shorter than the other
- the ball of the hip can be felt behind the buttocks or on the side of the hip (feels like a golf ball moves when the leg moves) (Picture 3, page 1)
Treatment and Follow-up
Radiologists review the x-ray to see how much of the ball of the femur is not covered by the socket of the pelvis. Nationwide Children’s Hospital has a standard way these x-rays are taken and reviewed by the radiologist. This process lowers the chance of mistakes. Based on these results, the providers decide how much follow up your child needs.
Orthopedic surgery may be recommended if there is a:
- big change in how much socket covers the ball over a short period of time
- only a little coverage of the socket over the femoral head
- change in your child’s physical exam
Hip surveillance can be done by any department at Nationwide Children’s. If your child’s hips stay stable and they have a low risk for hip dislocation, they can continue to be followed by their current provider. If you have concerns or your child has a higher risk for hip dislocation, they may be referred to an orthopedic surgeon for more evaluation and discussion.
HH-II-253 | Copyright 2020, Nationwide Children’s Hospital


