Resources for Professionals
By the Numbers: Interventional Cardiology
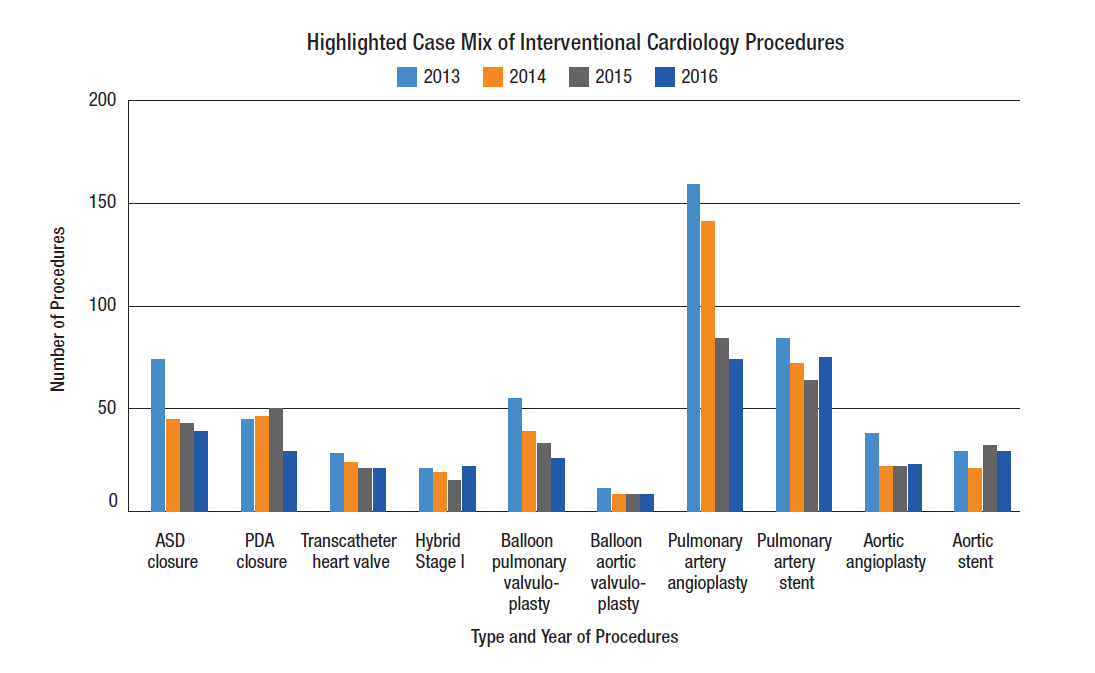
The Interventional Cardiology program is internationally recognized and provides a full spectrum of diagnostic and therapeutic cardiac catheterization procedures for all our patients — from neonates to adults.
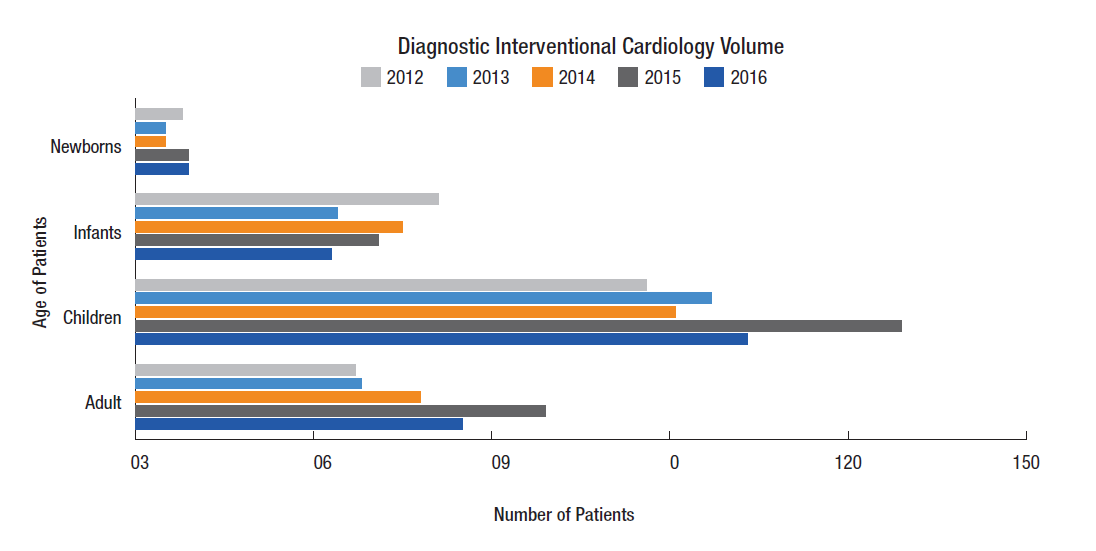
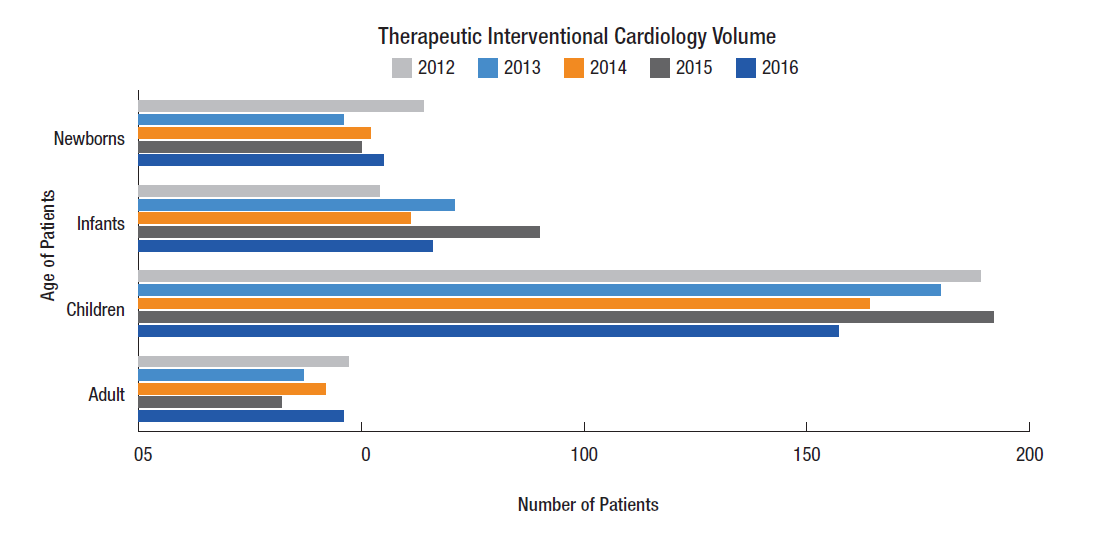
Because we use less-invasive modalities for diagnosis as often as possible, 87 percent of neonates who have catheterization procedures are getting therapeutic catheterizations.
We performed 508 therapeutic catheterizations in 2014.
According to the BCMH data, as a leader in the field, our catheterization volumes rank above the average of all Ohio hospital averages combined. We performed 418 pediatric therapeutic catheterizations in 2014. BCMH does not include adult patients in their data. We also performed 90 adult catheterizations as part of our ACHD program.
In 2014, The Heart Center performed 18 Melody procedures and 5 Native procedures.
The Heart Center is a leader in innovation, particularly in transcatheter pulmonary valve procedures. The Heart Center played a key role in the FDA approval of the Medtronic Melody® Transcatheter Pulmonary Valve and Ensemble Delivery System, as well as in the development of both the stent and balloon-in-balloon products. This procedure is used to replace deteriorating valves in existing conduits without additional open heart surgeries. Over the lifetime of a patient, this could reduce the number of open heart surgeries needed potentially from 8 to 3.
Now, The Heart Center is again on the cutting edge of innovation, as one of three institutions internationally participating in a clinical trial of the Native Outflow Tract Transcatheter Pulmonary Valve. The Native PV procedure would enable valve replacement in cases where the patient does not have a conduit already in place. Like the Melody procedure, it eliminates the need for repeat open heart surgeries for valve replacements after the initial open heart surgery.
Highlights in Quality: Interventional Cardiology
Concerns related to patient radiation exposure have led The Heart Center to create quality initiatives to reduce median radiation dosage during catheterization and electrophysiology (EP) procedures from 185 mGy in 2013 to 175 mGy in 2014. Through the increased use of collimation when appropriate, implementation a of color-coded dose tracking system (DTS), installation of new software, decrease in the frame rate to 10 fps when possible (based on patient weight), use of “Live Zoom” rather than “Radiological Zoom” and system alerts for staff, we reduced the year to date (YTD) median dose to 159 mGy by the end of 2014, exceeding our goals.
| 2014 | YTD Median Dose (mGy) | Quarterly Dose (mGy) |
|---|---|---|
| Q1 | 169.3 | 169.3 |
| Q2 | 176.9 | 177.0 |
| Q3 | 167.0 | 132.1 |
| Q4 | 159.0 | 142.0 |
Patients receiving high doses of radiation are at greater risk for radiation-related skin lesions. To address this concern, we initiated a quality initiative focused on obtaining at least 85 percent compliance in post-procedure skin assessment in cases of 3000 mGy or more of radiation exposure at discharge and at the follow-up clinic visit. By improving patient education regarding exposure on the day of the procedure, standardizing a questionnaire for follow-up clinic visits, training staff on detecting radiation injuries and optimizing use of clinical software for documentation and orders, we were able to achieve better-than-target compliance in the third and fourth quarters of 2014.
| 2014 | Skin Assessment at Discharge | Number of Patients | Assessment at 6-Week Clinic Visit |
|---|---|---|---|
| Q3 and Q4 | 86% | 7 | 100% |
| Total 2014 | 67% | 12 | 75% |
These reports feature a snapshot of quality initiatives and program outcomes from The Heart Center at Nationwide Children's Hospital.
2012 - Interventional Cardiology Quality Outcomes
We’ve cut the annual median radiation dosage in half.
To help lower the risk and amounts of exposure of radiation that our patients could potentially absorb, we carefully manage the dosage on a case-by-case basis to keep that exposure as low as possible.
In all radiation-required procedures, the benefit from the procedure should outweigh the potential risk of exposure. Dose management requires careful consideration during the procedure. The Cath Lab always strives to keep doses As Low As Reasonably Achievable (ALARA). ALARA reminds us to use the lowest possible dose while completing the procedure safely. “Step Lightly” is an initiative from the Alliance for Radiation Safety in Pediatric Imaging reminding us to always use pediatric-sized doses and to “Step Lightly” on the fluoroscopy pedal.
In The Heart Center, our aim in 2011 was to attain a median dose exposure per case that was ≤ 95 percent of the median dose of 374 mGy from the previous two years. The Cath Lab surpassed this objective by achieving a 2011 median case dosage of 221 mGy, which was 59 percent of the median case dosage in 2009-10. From January 2008 to December 2011, the Cath Lab has reduced the annual median dose of radiation by approximately 50 percent.
2010 - Interventional Cardiology Quality Outcomes
Quality improvement and risk adjustment: Participation in national and international quality improvement efforts including C3PO and MAGIC registries.
Publications
- Holzer RJ, Sisk M, Chisolm JL, Hill SL, Olshove V, Phillips A, Cheatham JP, Galatowicz M. Completion Angiography After Cardiac Surgery for Congenital Heart Disease: Complementing the Intraoperative Imaging Modalities. Pediatr Cardiol 2009;30(8)1075-82.
- Holzer RJ, Wood A, Chisolm JL, Hill SL, Phillips A, Galantowicz M, Cheatham JP. Atrial septal interventions in patients with hypoplastic left heart syndrome. Catheterization & Cardiovascular Interventions 72(5):696-704. 2008.
- Holzer R, Marshall A, Kreutzer J, Hirsch R, Chisolm J, Hill S, Galantowicz M, Phillips A, Cheatham J, L Bergerson. Hybrid Procedures: Adverse Events and Procedural Characteristics – Results of a Multi-institutional Registry. Congenital Heart Dis. 2010;5:233-242 (May-June 2010).
- Holzer RJ, Chisolm JL, Hill SL, Olshove V, Phillips A, Cheatham JP, Galantowicz M. "Hybrid" stent delivery in the pulmonary circulation. Journal of Invasive Cardiology. 2008;592-598.
- Galantowicz M, Cheatham JP, Phillips A, Cua CL, Hoffman TM, Hill SL, Rodeman R. Hybrid approach for hypoplastic left heart syndrome: intermediate results after the learning curve. Annals of Thoracic Surgery 85(6):2063-70; discussion. 2070;-1.
- Holzer RJ, Chisolm JL, Hill SL, Cheatham JP. Stenting complex aortic arch obstructions. Catheterization & Cardiovascular Interventions 71(3):375-82. 2008.
- Fu YC, Bass J, Amin Z, Radtke W, Cheatham JP, Hellenbrand WE, Balzer D, Cao QL, Hijazi ZM. Transcatheter closure of perimembranous ventricular septal defects using the new Amplatzer membranous VSD occluder: results of the U.S. phase I trial. Journal of the American College of Cardiology 47(2):319-25. 2006.
- Galantowicz M, Cheatham JP. Lessons learned from the development of a new hybrid strategy for the management of hypoplastic left heart syndrome.[republished from Pediatr Cardiol. 2005 Mar-Apr;26(2):190-9; PMID: 15906023]. Pediatric Cardiology 26(3):190-9. 2005;-Jun.
- Bacha EA, Cao QL, Galantowicz ME, Cheatham JP, Fleishman CE, Weinstein SW, Becker PA, Hill SL, Koenig P, Alboliras E, Abdulla R, Starr JP, Hijazi ZM. Multicenter experience with perventricular device closure of muscular ventricular septal defects. Pediatric Cardiology 26(2):169-75. 2005;-Apr.
- Holzer R, Balzer D, Cao QL, Lock K, Hijazi ZM, Amplatzer Muscular Ventricular Septal Defect Investigators. Device closure of muscular ventricular septal defects using the Amplatzer muscular ventricular septal defect occluder: immediate and mid-term results of a U.S. registry. Journal of the American College of Cardiology 43(7):1257-63. 2004.
- Holzer R, Balzer D, Amin Z, Ruiz CE, Feinstein J, Bass J, Vance M, Cao QL, Hijazi ZM. Transcatheter closure of postinfarction ventricular septal defects using the new Amplatzer muscular VSD occluder: Results of a U.S. Registry. Catheterization & Cardiovascular Interventions 61(2):196-201. 2004.
- Cheatham JP. The ideal cardiac catheterization laboratory: Not Just for Cardiologists Anymore … it is Hybrid Time! For textbook entitled Percutaneous Interventions for Congenital Heart Disease. Editors Horst Sievert, Shakeel A. Qureshi, Neil Wilson and Ziyad Hijazi, Informa Healthcare, Abingdon, UK. pp 3-11, 2007.
- Hill SL, Hijazii ZM, Hellenbrand WE, Cheatham JP. Evaluation of the AMPLATZER Vascular Plug for embolization of peripheral vascular malformations associated with congenital heart disease. Catheterization and Cardiovascular Interventions, 67:113-119, 2006.
- Cheatham JP. How to Build a Hybrid Congenital Heart Disease Program For textbook entitled Complications in Percutaneous Interventions For Congenital & Structural Heart Disease. Edited by Hijazi ZM, Feldman T, Cheatham, JP, Sievert H. Informa Healthcare, UK, pp 31-40, 2009.