Bladder Exstrophy
Treatment and care when the bladder is open and exposed on the outside of the abdomen.
Pioneering New Hope for Bladder Exstrophy Care
Meet Dr. Cuckow
What Is Bladder Exstrophy?
Bladder exstrophy is a rare condition when a baby's bladder sticks out through the wall of the stomach (abdomen). The bladder is flat and can be seen on the outside of the body. A typical bladder is round and located inside the lower part of the abdomen. In bladder exstrophy, the skin, muscles and hip (pelvic) bones don't join properly and the bladder can't hold urine.
Bladder exstrophy involves organs of the urinary tract, as well as the digestive and reproductive systems. Defects of the abdominal wall, bladder, genitals, pelvic bones, final section of the large intestine (rectum) and opening at the end of the rectum (anus) can occur.
Children with bladder exstrophy also have vesicoureteral reflux. This condition causes urine to flow the wrong way — from the bladder back up into the tubes that connect to the kidneys (ureters). Children with bladder exstrophy also may have epispadias. Epispadias is a condition where the tube that carries urine from the bladder (the urethra) does not fully close during development.
Bladder exstrophy and epispadias are part of a spectrum, or a group of related conditions. When only the penis in boys or the clitoris in girls is affected, it is called primary epispadias. When the bladder is also involved, it’s called exstrophy. Exstrophy is more common than primary or isolated epispadias. With exstrophy, the bladder is on the outside, and the penis or clitoris has an opening (that’s the epispadias part). So, in summary, you can have epispadias without exstrophy, but exstrophy always includes epispadias.
What Causes Bladder Exstrophy?
Bladder exstrophy is rare, occurring in one in 10,000-50,000 births. The exact cause is still not known. It happens during development, before birth. The most likely reason is due to family history. If a parent has bladder exstrophy, the risk of having a child with the condition is 1 in 70. If a family has a child with bladder exstrophy, there is a 1 in 100 chance of having a second child with the condition. The condition is more common among boys than girls.
What Are the Signs and Symptoms of Bladder Exstrophy?
The appearance of the bladder is the most obvious sign of bladder exstrophy. The bladder sticks out of an opening in the belly or it completely forms on the outside of the body. Other signs and symptoms include:
- The bladder is smaller and flatter than a typical bladder. It holds less urine
- The belly button is lower
- The anus is lower
- The pelvic bones don’t come together or may rotate outward
- In boys, the testicles don’t descend or may not be in the usual position
- Children with bladder exstrophy are totally incontinent. This means they can't control their urine flow
- Urine may be cloudy
For children with epispadias, signs and symptoms may include:
In males:
- Penis looks broad, short and curved upward
- Pelvic bones are wide apart
- Urethra opens on top of penis instead of at top
In females:
- Clitoris and labia look different
- Urethra opens toward clitoris or belly
- External genitalia may not form or function properly
How Is Bladder Exstrophy Diagnosed?
Bladder exstrophy may be diagnosed during pregnancy. Sometimes it is found during a routine ultrasound when the bladder may not be visible. In those cases, the care team will follow up with MRI (magnetic resonance imaging) for more detailed images of the bladder.
Around 16 to 20 weeks into pregnancy, there’s a routine ultrasound to see if everything is growing correctly. During this scan, doctors look for signs of exstrophy. Signs might include:
- Thickened Bladder Plate: They check if the bladder wall is thicker than usual.
- Low Set Umbilical Cord: They see if the belly button cord is in the right place.
- Epispadias Penis: In boys, they look for a penis that’s shorter, thicker and bends backward against the tummy.
If the doctors suspect exstrophy, more scans happen. The care team can work with the family to plan for the baby’s delivery and connect them with other families dealing with exstrophy.
About half of cases are not diagnosed until after birth.
How Is Bladder Exstrophy Treated?
Bladder exstrophy is treated with surgery which is done in stages. The first procedure, to close the bladder, is done once the baby is established on feeding and has started to gain weight, somewhere between 2 weeks and 3 months of age. Unlike most centers in the United States, at Nationwide Children's Hospital, we are often able to close the bladder without performing an osteotomy (cutting the hip bones to reshape and close the pelvis). Whether or not an osteotomy is done, children usually are in the hospital for 6-10 days.
The next step is called the Kelly procedure. This involves rebuilding the soft tissue of the bladder neck. It uses existing muscle and soft tissue to create the new neck of the bladder. This ring of muscle then works like a sphincter to open and close bladder. This helps to control the flow of urine. The Kelly procedure creates a sphincter because a natural one did not form. The Kelly procedure is typically done around 1-2 years of age and children are in the hospital for about 5-7 days.
Some boys will also need surgery to bring urethra, the tube through which urine flows, to the end of the penis.
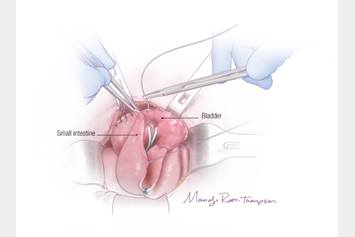
If a child has a small, unhealthy bladder that does not grow as the child gets older, a bladder augmentation may be needed. In this procedure, a piece of intestine is used to increase the size of the bladder. With the Kelly approach, the number of children requiring an augmentation is much less than with other techniques of exstrophy management.
What Will My Child's Life Be Like With Bladder Exstrophy?
Children born with bladder exstrophy will need surgeries to repair the birth defect. These surgeries will help:
- Gain bladder control (become toilet trained)
- Preserve kidney function
- Repair genital appearance
- Help gain sexual function
For many children (about 75%), the Kelly procedure is considered the most major operation to treat the condition. Additional treatments may include procedures to repair the appearance of the external genitalia, abdominal wall and control of their urine in the daytime. Nighttime continence may take longer to develop. In some of the boys, the end of the penis will need some further surgery to bring the urethra to its tip.
After surgery, doctors check how well the bladder is working. If your child has trouble staying dry, they might need more tests. These tests happen while the person is asleep (under anesthesia). Sometimes, doctors put “bulking agents” into the bladder. It helps the bladder hold urine better.
If More Surgery Is Needed
If your child still can’t stay dry, they might need another surgery. Here’s what it involves:
- Bladder Neck Reconstruction: Fixing the part where the bladder connects to other tubes.
- Ileocystoplasty: Making the bladder bigger using a piece of the intestine.
- Appendico-Vesicostomy (Mitrofanoff Channel): Creating a new way for pee to come out. It’s like a shortcut.
About 20% of patients might need this surgery. People who have this surgery will use a catheter (a thin tube) to empty their bladders regularly. It becomes part of their daily routine.
Ongoing care will help to make sure your child's bladder, kidneys and genitals develop and remain functioning in a healthy way. Many people regain continence after surgery and maintain it throughout their lifetime.
When Should I Seek Help?
Call the healthcare provider if your child has:
- Symptoms that don’t get better or get worse
- New symptoms
Why Choose Nationwide Children's to Treat My Child's Bladder Exstrophy?
When it comes to treating bladder exstrophy and epispadias in children, Nationwide Children's is the only hospital in the United States that is able to offer the Kelly procedure.
The Kelly procedure differs from the traditional surgical treatment for bladder exstrophy that involves a pelvic osteotomy. With an osteotomy, the child stays in the hospital, in traction, for up to 2 months. With the Kelly procedure, the child will stay at Nationwide Children's for about 8 days. After the procedure, continence develops over the next few years. The end goal is to have the child completely dry by the time they enter kindergarten.
The Bladder Exstrophy Program is led by Dr. Peter Cuckow. Dr. Cuckow is considered the global expert on this procedure that provides better continence outcomes. The pediatric Urology team at Nationwide Children's has extensive experience with complex urological reconstruction.
Can I Transfer My Child's Care to Nationwide Children's?
If your child is not diagnosed here, you can still request to speak with the team at Nationwide Children's. Even if your child had their first surgery at another pediatric hospital, it's never too late to connect with our team to learn about your child's options.
Leading the Way to New Treatments and Outcomes Through Clinical Research
Clinical care and research work together. This helps scientists and doctors to find new treatments and therapies. Clinical studies (also called clinical trials) will continue to become more common in daily care at Nationwide Children's. Clinical studies help doctors learn more about conditions and treatment.
This means you might hear about a clinical study that your child might be able to join. This does not mean that your child has to join a study. You always have the choice about whether or not to join a study.
Next Steps
We understand that this can be a difficult time. At Nationwide Children's, our team is here to support you and your family every step of the way.
New Patients
Whether you have a child that was newly diagnosed with bladder exstrophy, you want to explore all your options, or you are in need of a revision, our team is here to help. Call us at (614) 722-6250.