Hypoplastic Left Heart Syndrome (HLHS)
Hypoplastic left heart syndrome is a condition where the left side chambers of the heart develop too small to work effectively.
What Is Hypoplastic Left Heart Syndrome (HLHS)?
In HLHS, the parts on the left side of the heart do not develop all the way and are too small (hypoplastic). These parts include:
- The mitral valve
- The left ventricle
- The aortic valve
- The aorta
When the left lower pumping chamber (left ventricle) is smaller, it can’t get enough oxygenated blood to the body. Babies with HLHS will have an atrial septal defect (ASD) and a patent ductus arteriosus (PDA) to get oxygenated blood (blood in red in the image) out to the body and brain.
In rare cases, an unborn baby with severe HLHS may have no ASD. This is called HLHS with an intact atrial septum. This can be very dangerous since there is no opening between the left upper chamber (left atrium) and the right upper chamber (right atrium). Blood returning from the lungs cannot get out of the chamber. This can cause lung damage and makes treating the heart problem more difficult.
What Causes Hypoplastic Left Heart Syndrome?
In most cases, parents have no control over their baby’s condition and have not done anything to cause the problem. In many cases, the cause of congenital heart defects is unknown. If you have specific questions or concerns about you or your baby, talk with your doctor or nurse practitioner.
Diagnosis of Hypoplastic Left Heart Syndrome
When you are pregnant, there are many tests that can tell the doctor if your baby has a heart (cardiac) problem. However, some problems can’t be seen until after your baby is born. The following are some prenatal tests that may be done:
- Prenatal ultrasound: Complex heart defects are usually found during a pregnancy (prenatal) ultrasound. This test tells us if your baby’s heart is not shaped the right way. If this is found, you will be scheduled for a fetal echocardiogram to get more information.
- Fetal echocardiogram: A fetal echocardiogram is a special ultrasound used by a pediatric heart doctor (cardiologist). This test looks closely at your baby’s heart and surrounding blood vessels. The cardiologist will assess your baby after birth with an echocardiogram to confirm the diagnosis.
After Your Baby Is Born (Postnatal Diagnosis)
- Echocardiogram: An echocardiogram is a special ultrasound used by a pediatric heart doctor (cardiologist) to look closely at your baby’s heart and surrounding blood vessels.
- Heart Catheterization: This is a test to measure pressures in the heart. It can also take pictures of the heart and open a narrowing with a balloon or small metal coil, called a stent. Heart catheterizations are done while your child is asleep with medicines called anesthesia.
- Cardiac MRI: A test that uses radio waves, magnets, and a computer to make detailed pictures of the heart and blood vessels. Cardiac MRI can provide detailed information on the type and severity of heart disease.
Other Tests:
Some congenital conditions are caused by a baby’s DNA. The doctors may suggest genetic testing to find out more about this. DNA is made up of information inside your baby’s cells that make them who they are, like blueprints for a house.
- Cell-Free Fetal DNA Testing: A sample of blood is taken to look for copies of your baby's (fetal) DNA. A positive result means that there could be problems with the DNA. This must be confirmed with another test to be sure of the result. Other testing may be done before or after birth, depending on your baby’s needs.
- Amniocentesis: A small sample of amniotic fluid that surrounds the baby in the womb is taken and tested for DNA problems. This test is usually done in the middle of the second trimester of pregnancy, usually between 14 and 20 weeks. It can be used to confirm findings from the cell-free fetal DNA test.
- Karyotype or Microarray: A sample of your baby’s blood is taken to test for DNA problems. This is called either a karyotype (basic chromosome study) or a microarray (more detailed look at all genes).
How Hypoplastic Left Heart Syndrome Is Treated
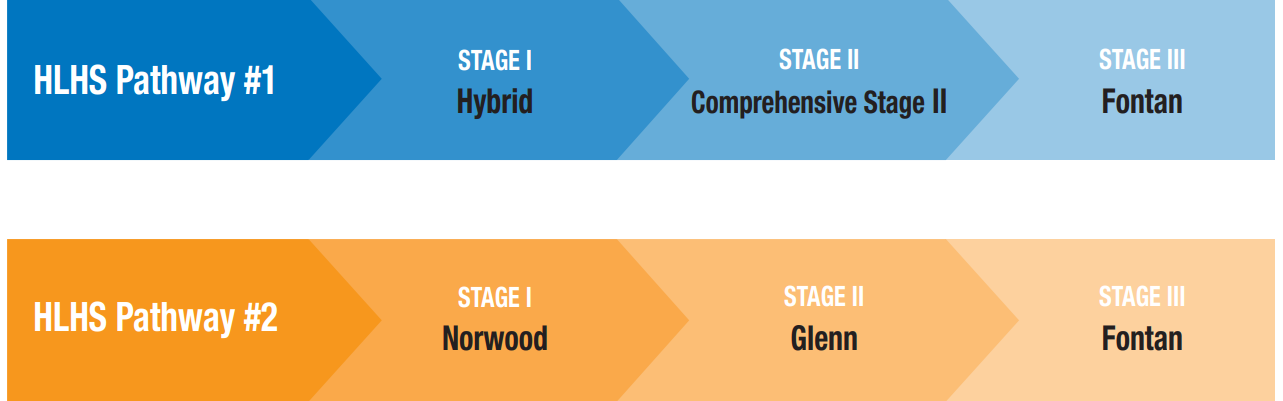
Children born with HLHS all need several surgeries to live. The surgeries are done in stages over the first few years of life. The first surgery is usually in the first week of life. Each stage plays an important step to reroute the blood flow of the heart around the small poorly developed parts. While most babies do well with the surgeries, the surgeries are not able fix the heart and make it normal again. HLHS is a lifelong heart problem. The goal is to balance the blood flow so your child can grow and develop. Even with the best medicines and surgeries, there is still a risk of heart failure and possible death.
There are 2 possible surgical pathways for HLHS. The specific pathway for your baby will depend on the details of their heart defect at birth.
Care During Your Pregnancy
If a test finds that you are carrying a baby with a heart defect, you will still get care from your pregnancy doctor (obstetrician). They may refer you to a maternal-fetal medicine (MFM) specialist or the Fetal Center at Nationwide Children’s. They will help you connect with a team of fetal experts. At the Fetal Center, you will meet with a multidisciplinary team including cardiologists (doctors who specialize in babies' hearts), neonatologists (doctors who specialize in treating newborns), cardiothoracic surgeons (doctors who perform surgery), and nurses. They will help you learn more about your baby’s care after they are born. Nurse coordinators can answer your questions, guide you through your pregnancy, and prepare you for what to expect.
During clinic visits, the medical team will discuss the diagnosis, treatment, recovery, and long-term outcome for your baby. You will get a tour of the Cardiac Intensive Care Unit so you know what to expect during the hospital stay.
Your doctor will watch your pregnancy closely. You will deliver your baby at a hospital that is ready to care for babies like yours. Talk to your obstetrician about your plans for labor and delivery. Contact your doctor right away if you have any concerns.
Fetal surgery may be an option. This is done during pregnancy. Fetal surgery may help a small number of babies with single ventricle heart defects. Your medical team will talk about the risks and benefits if this is an option for your unborn baby.
Care After Your Baby Is Born
At the delivery hospital, a doctor who specializes in working with sick infants (neonatologist) will manage the care of your baby. They will watch your baby’s breathing and heart rate and look for other problems. Babies born with heart defects may need care in the Neonatal Intensive Care Unit (NICU) at the delivery hospital. An intravenous line (IV) may be started in your baby’s belly button (umbilicus), arm, leg, or scalp. It will give fluids, medicines, and antibiotics to prevent dehydration and infection.
Your baby may need help with breathing, extra oxygen. Your baby will need to be started on a medicine called prostaglandin E (PGE, or "prostins"). This medicine keeps the blood flowing through the patent ductus arteriosus (PDA). Keeping the PDA open lets blood flow to your child’s lungs or body, helping to keep them stable until surgery.
Your baby will need to be transferred to Nationwide Children’s Hospital Cardiothoracic Intensive Care Unit (CTICU) shortly after birth by the Nationwide Children’s Mobile Intensive Care team. The team is experienced at moving newborns with heart defects. Every effort is made to let you hold and see your baby before they leave the birth hospital.
At Nationwide Children’s Hospital, you will meet with a team of many different specialists. This team includes:
- Cardiologists: Doctors who specialize in working with the heart
- Cardiothoracic surgeons: Doctors who specialize in surgery on the heart and lungs
- Neonatologists: Doctors who specialize in treating newborns
- Interventional cardiologist and catheterization team: A team of health care professionals that specialize in heart procedures
- Other specialized support, like social work, nutrition, therapy, psychology
- A specialized team of nurses and nurse practitioners
Pre-Operative Care and Testing (For Surgical Treatment)
When your baby gets to the CTICU at Nationwide Children’s Hospital, they will have many tests. These tests include an echocardiogram and an EKG. These tests will help the team make a plan for your baby at the Heart Center Case Management Conference. This plan includes choices about surgeries, procedures, and timing.
Depending on your baby's heart problem and the timing of surgery, they may need a long-term IV called a peripherally inserted central catheter (PICC). It can give medicines and a form of nutrition called total parenteral nutrition (TPN). Blood can also be drawn from the PICC so your baby doesn’t need to be stuck as often.
Because all of the organs are developing at the same time, it is important to check your baby for other problems. A head ultrasound (HUS) will be done in the first few days after birth to look for any brain problems, such as bleeding. An ultrasound of the kidneys (renal ultrasound) will also be done to make sure they are healthy.
Conserving Blood
The Heart Center at Nationwide Children’s Hospital has special methods to save (conserve) as much blood as possible during surgery. This can decrease the need for a blood transfusion later. These methods include:
- Saving your child’s blood lost during surgery to use after surgery
- Using a shorter cardiopulmonary bypass circuit
- Using the smallest amount of blood needed for lab tests
- Increasing time between lab tests
- Stopping lab tests when possible
Care After Surgery
After surgery, your baby will go to the Cardiothoracic Intensive Care Unit (CTICU). They may be on a breathing machine and have many tubes, wires, and equipment to keep them stable and make sure they are okay. Members of their health care team may make changes to your baby’s medicines and breathing machine often. This will happen the most in the first 24 to 48 hours after surgery.
Other treatments your baby will probably get after surgery are:
- Antibiotic medicine to prevent infection
- Fluids and nutrition through an IV or PICC line
- Heart medicines by IV or by mouth
- Chest drainage tube
- Oxygen
- Pain medicines
- A tube in the nose to the stomach (nasogastric [NG] tube) to keep the stomach empty
- Blood transfusions, when needed
Feeding Your Baby
For all babies, growth and nutrition are an important part of their care. Your baby will be able to eat as soon as they are stable and safe. This may be the first chest/breastfeeding in the delivery room, or it may be after surgery. For all parents interested in giving their own milk, we encourage and support this. Some babies may need to start with small amounts of milk at first and slowly increase. Babies with heart defects may tire easily while feeding or have trouble sucking and swallowing. A temporary feeding tube may be placed into your baby’s nose or mouth, down into the stomach. Some babies will need early nutrition through an IV, called total parenteral nutrition (TPN).
Your medical team will help you decide on the safest feeding approach. Lactation nurses and occupational and speech therapists can work with your baby on oral feeding skills. They can also help you with pumping or direct chest/breastfeeding, when needed. Your baby may go home eating by mouth, but some babies may need help getting the calories needed to grow.
At first, your baby is expected to gain between 20 to 30 grams per day once they reach their goal feedings. Your dietitian will watch this and change the feeding plan and calories as needed.
Feeding Problems
It is common for babies with heart problems to struggle with feeds. This is called feeding intolerance. Symptoms may include fussiness, swollen belly, throwing up (vomiting), poor weight gain, blood in the poop (stool), or loose, runny stool.
Milk protein allergies can be one cause of feeding intolerance. This can be fixed by changing formula. It can also help if the parent giving their own milk stops eating and drinking milk products.
Gastrostomy Tube (G-tube/Feeding Tube)
If your child can’t safely eat enough by mouth in order to grow, they may need a G-tube. A G-tube is a thin, flexible tube that goes through the skin and into the stomach. Liquids, like milk, water, and medicines, go right into your child’s stomach through this tube. The G-tube can be easily removed once it is no longer needed.
Discharge Planning
Your baby will go to the cardiac step-down unit (H4A) when they are off the breathing machine and can handle heart medicines and feedings. Here, your baby will recover, learn to eat, and start to breathe without oxygen. Your baby will go home once their oxygen levels are good and they are gaining weight. This can take at least 3 to 4 weeks after surgery or longer. The total time your baby will stay in the hospital depends on if they were born early or if there are other problems.
You will have a discharge call with your pediatrician, cardiologist, nurses, and dietitians before going home. This helps your pediatrician know what is going on with your baby before their first doctor’s visit. It also gives you time to ask questions. Hospital staff will make sure you and your baby are ready for home and support for their continued care. Social workers can help with resources. Our psychologist and chaplains will continue to support you on the step-down unit. .
Discharge Education
You will need to:
- Do CPR training in the Columbus Blue Jackets Family Resource Center before you leave.
- Be able to give well-baby care, feed your child, and understand the medicines that your baby is taking.
- Know the signs and symptoms to watch for at home and when to call and when to bring your child directly to the hospital.
Tests Before Going Home
- Hearing screen: The state requires that all babies must have a hearing screen before going home for the first time.
- Newborn screening: This test is sometimes called a PKU test. It is a lab test done during the first 24 hours of life. It looks at your baby’s blood for many serious but rare medical conditions. If it is not treated, these conditions can lead to slow growth, developmental disabilities, and possible death. Finding and treating these conditions early may prevent serious problems in the future.
- Hepatitis B vaccine: We encourage all parents to have their baby get the hepatitis B shot (vaccine) before going home for the first time. Your child’s pediatrician will give you the schedule for other vaccines.
- Car seat test: This test makes sure your baby’s heart rate, breathing, and oxygen levels are stable while in the car seat. Your baby will need to sit in the car seat with a monitor on for a set amount of time before going home.
- Cardiac tests: Your baby may have a discharge chest X-ray, echocardiogram, and EKG before being sent home.
Looking Ahead
Your baby will, likely, have pediatrician appointments every 2 months for well-baby checks and immunizations. They will work with the heart team to care for your baby.
Your cardiologist will follow up with your baby’s heart needs even after they are discharged from the hospital.
Future Pregnancies
Most of the time, congenital heart defects don’t happen again with future pregnancies. However, it is recommended that you meet with a geneticist, maternal-fetal medicine doctor (high-risk), or obstetrician before getting pregnant again. Your child’s cardiologist can also help answer questions. They can help you find out if you are at high risk of having another child with a heart defect. They can also talk with you about options and testing.
Next Steps
Care needs change as your child grows. At Nationwide Children’s Hospital, we are committed to providing the best care and quality of life for children of all ages, from in utero to adulthood and beyond.
For Expectant Parents With a Prenatal Diagnosis
Our expert team of fetal medicine specialists is here to guide and support you each step of the way.
For Parents of Children and Newborns
As the leader in pediatric care, The Heart Center offers cardiology services, cardiothoracic surgery, and everything else you would expect to find at a nationally-renowned heart center.
Learn more about The Heart CenterFor Adolescents and Adults
Adolescents and adults with congenital heart disease have different considerations than children. Our program was created to meet the medical and surgical needs of this unique and complex population.
Learn more about the Adolescent & Adult Congenital Heart Disease (ACHD) Program


