Giant Neck Mass (Cervical Teratoma)
A giant neck mass is an abnormal growth of the neck. There are two different types of masses including cervical teratomas and lymphatic malformations.
What Is a Giant Neck Mass?
A giant neck mass is a growth in or around the neck. After your child is born, the neck mass can cause breathing and swallowing problems.
The two most common kinds of neck masses are cervical teratomas and veno-lymphatic malformations.
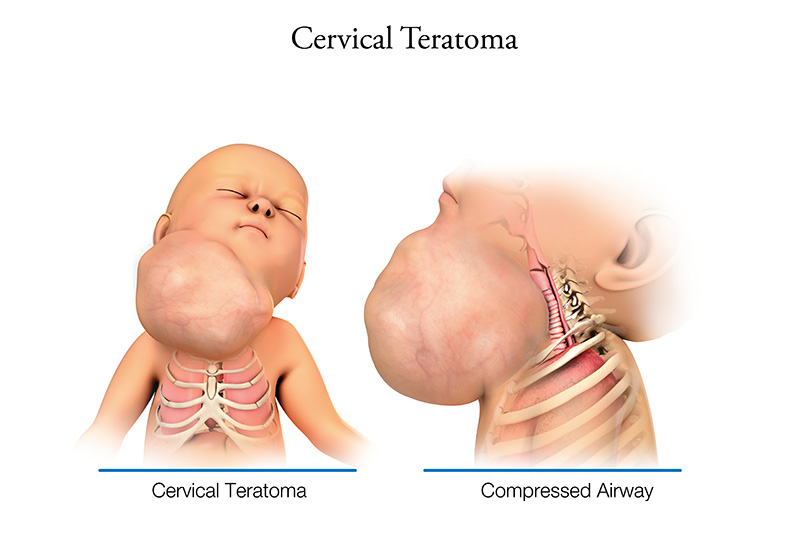
- Cervical teratomas - A cervical teratoma is a very rare tumor that is, often times, not cancer. It is part solid and part fluid. These tumors can be large, so they may cause changes to how your baby’s neck and face look and function. They can also make it hard for your baby to breathe and swallow.
- Lymphatic or vascular malformations – These include cystic hygroma or lymphatic malformation. These are a group of lymph vessels that form a growing, spongy mass of cysts. Lymphatic malformations are not cancer. The lymphatic system does many jobs for your body. This includes helping your immune system function and draining extra fluid from tissues. These tumors can spread to other parts of the body. In the neck, they look like a big mass.
Finding this condition during pregnancy and treating it early increases your baby’s chances of living. Depending on the type of neck mass and other body parts involved, your baby may need more than one surgery.
What Causes a Giant Neck Mass?
The cause of a giant neck mass is not known. They aren’t passed on by parents to their child, and they do not run in families. In most cases, the giant neck mass happens only one time. However, certain genetic problems can change how the lymphatic system forms. This increases the risk of having a giant neck mass.
What Are the Signs and Symptoms of a Giant Neck Mass?
During pregnancy, the mass could block your baby’s trachea (airway) and esophagus.
This could lead to a couple different problems:
- If the esophagus is blocked, your baby will have a hard time swallowing amniotic fluid. This could lead to too much amniotic fluid in the womb, causing early labor.
- If your baby’s airway is blocked, they may not be able to breathe in amniotic fluid. This could lead to lungs that are not as developed as they should be at birth.
How Is a Giant Neck Mass Diagnosed?
Giant neck mass is usually found (diagnosed) with an ultrasound during pregnancy. Your baby’s neck may look bent or over-extended. The doctor might be able to see the abnormal tissues in the neck.
Later in pregnancy, the ultrasound may show other problems, like:
- Extra amniotic fluid.
- An empty or small stomach. This could mean your baby can’t swallow amniotic fluid.
You may have other tests to help your doctors see if there are other problems with your baby’s airway or esophagus. These include a:
- Detailed fetal ultrasound: A special ultrasound to confirm the diagnosis and look for other problems.
- Fetal echocardiogram: A special ultrasound done to check on the blood vessels around your baby’s heart. It is done by a pediatric heart doctor (cardiologist).
- Fetal MRI (magnetic resonance imaging): A non-invasive imaging test that can look closely at your baby’s organs. It shows things that the ultrasound cannot.
Genetic Tests
Some congenital conditions are caused by a baby’s DNA. DNA is made up of information inside your baby’s cells that makes them who they are, like blueprints for a house. Doctors may suggest genetic testing to find out more about their DNA.
- Cell-Free Fetal DNA Testing: A sample of blood is taken to look for copies of your baby's (fetal) DNA. A positive result means that there could be problems with the DNA. This must be confirmed with another test to be sure of the result. Other testing may be done before or after birth, depending on your baby’s needs.
- Amniocentesis: A small sample of amniotic fluid that surrounds the baby in the womb is taken and tested for DNA problems. This procedure is usually done in the middle of the second trimester of pregnancy, usually between 14 and 20 weeks. It can be used to confirm findings from the cell-free fetal DNA test.
- Karyotype or Microarray: These tests are done with a sample of amniotic fluid or placenta before your baby is born. They can also be done after birth with a blood sample from the umbilical cord. They both check for DNA problems. A karyotype is a basic chromosome study and a microarray is a more detailed look at all genes.
Care During Your Pregnancy
If you are carrying a baby with a giant neck mass, you will keep getting care from your obstetrician (OB/GYN). They may refer you to The Fetal Center at Nationwide Children’s Hospital. There, you will work with a team that includes:
- Maternal-Fetal medicine doctor
- Neonatologists: Doctors who take care of newborns
- ENTs: Doctors who work with the ears, nose, and throat
- Interventional radiologists: Doctors who do treatments using imaging tests
- Geneticists and genetic counselors: Experts in medical genetics and counseling
- Nurses: Help care for your baby and teach you how to care for your baby
- Nurse coordinators: Guide you through your pregnancy and prepare you for what to expect
Ultrasounds will be done for the rest of your pregnancy to watch the mass's growth and the amniotic fluid. Your doctor will watch your pregnancy closely. You will deliver your baby at a hospital that is ready to care for high-risk babies like yours. Talk to your OB/GYN about your delivery plans. Contact your doctor right away if you have any concerns.
Delivery With Giant Neck Mass
If your baby’s airway is blocked by the mass when it is time for you to have the baby, an ex-utero intrapartum treatment (EXIT) procedure may be needed. During the EXIT procedure, you will have general anesthesia and a C-section. Only your baby’s head and arms will be delivered. The placenta and umbilical cord will stay attached, so the baby can still get oxygen-rich blood. Delivering this way lets the doctor put a breathing tube in your baby so they can breathe after the cord is cut. This tube may either be:
- Endotracheal tube – Goes in the mouth and down to the airway (trachea).
- Tracheostomy tube – A tube that goes into the airway (trachea) through a cut in the neck.
Your baby’s doctor will talk with you about long-term options for breathing and eating. They may need more than one surgery to treat the giant neck mass.
Care After Birth
- At the delivery hospital, a neonatologist will take care of your baby. Depending on whether or not your baby had an EXIT procedure will determine their care and timing of care.
- If your baby needs a breathing tube after they are born, they will be on a breathing machine (ventilator) to help their lungs work. If your baby cannot fully breathe on their own after birth, a breathing tube and ventilator will be needed to help their lungs work.
- Your baby may need to get a nasogastric (NG) tube in their nose or orogastric (OG) tube in their mouth. These tubes go into the stomach to feed your baby.
- Your baby will have intravenous (IV) lines to give them fluids and medicines. An arterial line will be in place to check blood pressure. Some of the medicines your baby gets will help with infection, blood pressure and pain.
- Your baby will go to the Neonatal Intensive Care Unit (NICU) at the main campus of Nationwide Children's Hospital right away for their care.
- We hope you will start pumping breast/chest milk for your baby right away. While some babies may not be able to start taking breast/chest milk right after birth, it is important to start pumping so your milk supply comes in. Lactation consultants can help you at your delivery hospital, and in the NICU.
How Is a Giant Neck Mass Treated?
After birth, your baby will be taken to the Nationwide Children’s Hospital main campus NICU for more testing and treatment. The Nationwide Children’s Hospital Lymphatic Malformations Team works with the NICU to care for babies with giant neck masses. Sometimes, the mass can’t be fully removed. It can be treated over time to help with swallowing and breathing.
These treatment options will be based on your baby’s symptoms:
- Surgery: Babies with giant neck mass may need surgery to have them removed.
- Sclerotherapy: Lymphatic malformations with large cysts inside the mass can’t usually be removed with surgery. These cysts must be drained and get injections to shrink the mass. This is called sclerotherapy. This therapy may need to happen over a longer period of time.
In many cases, the mass may keep your baby’s thyroid gland from growing partly or at all. If this happens, take medicine for a condition called hypothyroidism. This is a condition they will have forever.
Care After Surgery
After surgery, your baby will stay in the NICU.
Other treatments your baby will most likely need after surgery are:
- Antibiotic medicine to prevent infection.
- Pain medicines, as needed.
- Fluids and nutrients through an IV.
Feedings
Babies cannot breast/chest feed or take bottles until they are off the breathing machine. Once they are off the machine, it may take some time for them to learn to take milk or formula. They will start with small amounts of breast/chest milk or formula. The amount will slowly increase over time. Your baby may still be fed through the OG/NG tube while learning this skill. Some babies may need to go home with a long-term feeding tube called a gastrostomy tube (G-tube). This tube is put in through the wall of the belly into the stomach with surgery.
Discharge Planning
The time your baby is in the hospital will depend on their condition, their treatment, and how they heal. You will be able to take your baby home when:
- They can take enough formula or milk to grow and gain weight.
- There is a safe plan for supporting breathing outside of the hospital.
If your baby needs a feeding tube, tracheostomy, or other medical support at home, you will get education so you are ready to take care of your baby at home.
Looking Ahead
Your baby will need regular follow-up appointments to check their growth, development, and nutrition. Find a local pediatrician (doctor who specializes in the care of children) for check-ups, immunizations, and sick visits. Ask your program coordinator if you need help.
Your baby may also have follow-up appointments long-term to make sure the mass does not come back. In most cases, your child can live a long life. Your baby will also need to follow up with the ENT doctor, pediatric surgery team, lymphatic malformations team, and neonatal follow-up clinic. If they have other problems, they will need to see doctors and health care providers for those problems, as well.


