Velopharyngeal Dysfunction (VPD)
![]()
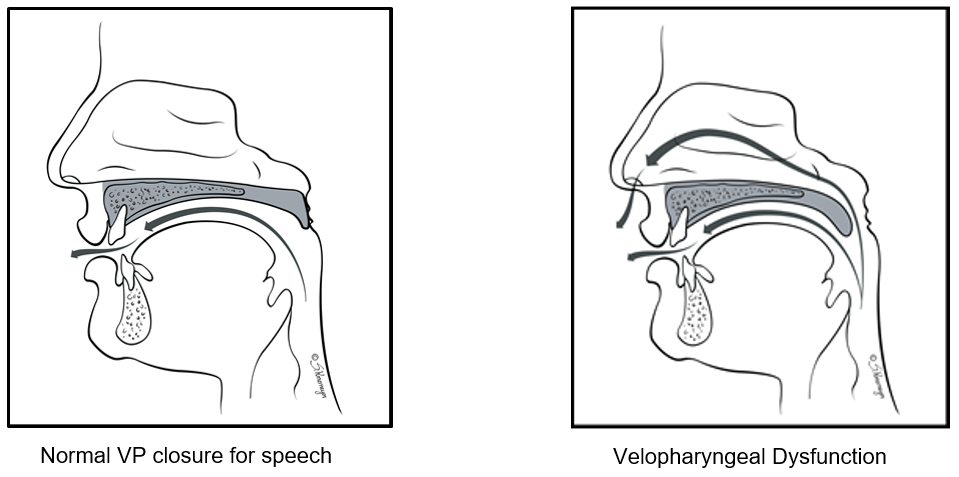
Velopharyngeal dysfunction (VEE lo fa RIN jee uhl dis FUNK shuhn), or VPD, occurs when the soft palate cannot separate the back of the mouth from the nose during speech, swallowing, or both. VPD can be caused by structural (anatomy) differences in the soft palate (roof of the mouth) and pharynx (throat), or muscular causes (such as weakness or poor coordination). Children with VPD often have very nasal speech, with air leaking through the nose as they talk. In some cases, the child has a hard time pronouncing words.
Cause
Some of the common causes of VPD are:
- A short soft palate that cannot reach the back of the throat
- A mismatch between the length of the palate and the depth of the throat, so the palate cannot reach the back of the throat
- Limited muscle function, weakness or an uncoordinated soft palate.This means the palate may be long enough but is unable to move high or far enough.
Some of the risk factors for VPD are:
- Cleft palate
- Certain syndromes, such as 22q11.2 deletion syndrome
- Some diseases of the central nervous system
- Muscle weakness caused by certain conditions
- Some children have more risk of VPD after having an adenoidectomy, if they have any of the above risk factors
Signs and symptoms
- Very nasal speech quality
- Air leaks through the nose while speaking
- Speech sounds weak or muffled
- Words not clearly spoken
- Food or liquid leaks through the nose while eating or drinking
Diagnosis
If VPD is suspected, your child will see a speech-language specialist and a surgeon to be evaluated and confirm the diagnosis. Children typically have a speech evaluation, which means special tests to measure nasality and imaging, if it is needed. (For more information, see Helping Hand HH-I-444, Nasopharyngoscopic Evaluation of Velopharyngeal Closure during Speech or HH-III-148, Multiview Speech Fluoroscopy.) The surgeon and speech pathologist will also examine your child’s mouth.
Speech sound (articulation) testing may also be done. During the speech evaluation and any imaging procedures, the child needs to attempt to say enough sounds or words to let us decide if speech symptoms of VPD are present.
In some cases more testing, such as an MRI, sleep study, or genetic testing, may be needed before the cause of VPD or the treatment plan can be finalized.
The diagnosis and treatment of VPD requires a team approach. The team includes a specially-trained speech-language pathologist and a surgeon, and sometimes additional healthcare providers, if needed.
Treatment
VPD is a treatable condition. Treatment options may include the following:
- Surgery is typically the first-line approach to treatment of VPD. There are several surgical treatments commonly used. Your child’s surgeon will choose which one is right for your child. Surgical management of VPD is very effective. It aims to improve speech by reducing the leakage of sound and airflow through the nose while the child is talking. The expected result of speech surgery is speech that is both easier to understand and more socially acceptable.
- Many children with VPD will also need speech therapy. The treatment team will decide if your child needs speech therapy, surgery or both.
- Rarely, a speech prosthesis may be an option to treat VPD. This is more common in people with a history of head or neck cancer, severe motor disorders or other complex medical situations.
HH-II-240 9/19 | Copyright 2019, Nationwide Children’s Hospital


