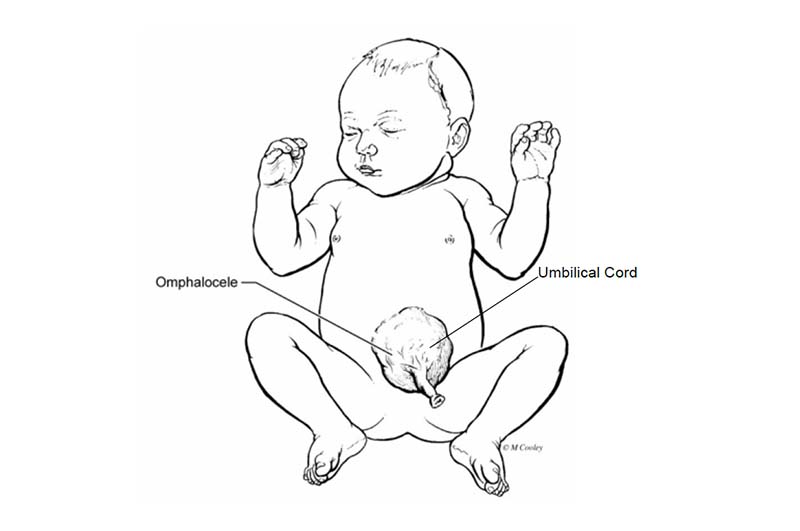
Omphalocele
An omphalocele is an abdominal wall defect that allows the intestine to remain outside the abdomen. An omphalocele can contain parts of the intestine, liver and other organs. The goal of surgery is to place the abdominal organs back into the baby’s body and repair the defect in the wall of the belly.
What is an Omphalocele?
Sometimes during pregnancy, the baby’s abdominal wall does not close at the umbilicus. The intestine remains outside the abdomen in a sac. This is called an omphalocele, which is an abdominal wall defect. An omphalocele can be small, containing parts of the intestine, or larger containing parts of the liver and other organs.
What Causes an Omphalocele?
The cause of an omphalocele is not known. It is congenital meaning it happens before your baby is born. Omphalocele develops in 1 in about every 5,000 live births. Approximately 25-40 percent of infants with an omphalocele have other birth defects such as genetic problems and heart defects. Many babies with omphalocele have an underlying genetic disorder. The survival rate for babies with omphalocele depends on the size of the defect, whether the baby is born premature, sac ruptures or if there are other problems.
Some babies born with omphalocele also has a condition called Beckwith-Wiedeman Syndrome (BWS). BWS is a condition where the baby has a large tongue, (macroglossia), which may interfere with breathing, swallowing, and speaking. Other problems with BWS include large abdominal organs (visceromegaly), low blood sugar (hypoglycemia) and kidney abnormalities.
How is Omphalocele Diagnosed?
Omphalocele may be found during routine prenatal ultrasound. If your doctor suspects a problem, additional tests may be ordered. These may include:
- Fetal MRI – a non-invasive imaging technique to help provide additional details of the baby’s organs that may not have been visualized on ultrasound
- Fetal echocardiogram – a specialized ultrasound to evaluate the baby’s heart structure and function
Other Tests
Some congenital conditions are because of changes in DNA, or a baby’s genetic make-up. The doctors may suggest genetic testing to find out more about your baby’s DNA.
- Cell-Free Fetal DNA testing – Your doctor can take a sample of your blood to look for copies of fetal (baby) DNA. This is only a screening test. A positive result means that there could be problems with the DNA. This should be confirmed with another test to be sure of the result. Other testing can be done before or after birth depending on the needs of the baby.
- Amniocentesis – A small sample of the amniotic fluid that surrounds the baby in the womb is taken and tested for DNA problems. This test is usually done in the middle of the second trimester. An amniocentesis can be used to confirm findings on the cell-free fetal DNA test.
- Testing the baby – After birth, a test is done with a sample of your baby’s blood to look for chromosome problems. This is called either a “karyotype” (basic chromosome study), or microarray (a more detailed look and all genes).
Care After Your Baby is Born
At the delivery hospital, a neonatologist (a doctor who specializes in treating newborns) will manage the care of your baby. The neonatologist will assess your baby’s breathing and heart rate, and examine the baby for other problems.
- Your baby will receive care in the delivery hospital’s neonatal intensive care unit (NICU).
- A breathing tube will be placed if your baby is having difficulty breathing.
- The omphalocele sac will be covered with a warm, moist sterile dressing.
- A tube will be put through your baby’s nose (nasogastric, NG) or mouth (orogastric, OG) down into the stomach. This tube helps to keep the stomach and intestines empty and decompressed.
- An intravenous line (IV) will be started in your baby’s arm, hand, foot or scalp. The IV provides fluids and antibiotics to prevent dehydration and infection.
- Your baby will be transferred to the main children’s hospital NICU for further care.
How is Omphalocele Treated?
- Your baby will not be able to drink breast milk or formula until after the intestines have healed from surgery. A special IV called a PICC (Peripherally inserted central catheter) will be used to give your baby IV nutrition called TPN (total parenteral nutrition). TPN has all of the calories and nourishment needed for your baby to grow.
- We strongly encourage you to pump breastmilk to provide to you baby when he or she is ready to start feeds. Breastmilk is best for all babies, and is particularly important for babies with omphalocele, as breastmilk is very gentle on the intestines.
- The NG or OG will stay in place through the time of surgery, and after surgery until the intestines recover and start to function well
- Ultrasound of the heart, kidneys and brain will be done
Surgery
Once your baby has been admitted to the NICU, the pediatric surgery team will evaluate the omphalocele and decide on which surgical approach would be best. The goal of surgery is to place the abdominal organs back into the baby’s body and repair the defect in the wall of the belly.
Primary Repair - Babies born with a small omphalocele will have surgery a couple days after birth. The surgeon places the organs that are inside the omphalocele back into the abdomen. The muscle and skin are closed. If a baby has a large omphalocele and small abdomen, the abdominal muscle cannot be sewn together. Instead, the hole in the muscle is covered with Gore-Tex (an absorbable material) and the skin is closed over it.
Staged Repair - If the baby has a large omphalocele the surgery may be done in stages. The omphalocele sac is removed and a surgical pouch called a silo is placed around the intestines and liver. It is suspended over the baby. Slowly, over time, the intestines and liver are pushed back into the abdomen. This can take a few days or weeks. Surgery will be done right away if the sac breaks. When the intestines and liver can comfortably fit within the abdominal cavity, the silo is removed and the hole in the abdomen is closed.
Sometimes the omphalocele is so large that the organs cannot be placed back inside the baby’s abdomen. In this situation the surgeon feels it is best to wait until the child is older to repair the omphalocele. During this stage you will take your baby home and have close follow up with the pediatric surgeon. Every day the omphalocele is wrapped. The wrap will apply pressure over the sac so that the omphalocele is reduced in size. Eventually skin will grow and cover around the omphalocele.
Care After Surgery
After surgery, your baby will receive care in the hospital’s NICU. Your baby will need to be on a breathing machine until he or she is fully recovered from surgery. Other treatments your baby will probably need after surgery are:
- Antibiotics to prevent infection
- Fluids and nutrients given through CVL
- Oxygen
- Pain medicines as needed
- The NG or OG tube will stay in place until your baby’s intestines begin to work properly. This may take several weeks. Your baby will not be able to eat until the intestines have healed
Feeding
Feedings are started once the intestines are fully healed after surgery. When it is time to feed your baby his or her first bottle, the NG or OG tube will be removed. Your baby will be started off with small amounts of formula or breast milk, and the amount will be increased gradually over time. When your baby is taking enough formula or breast milk to grow and gain weight, the IV will be removed.
Complications
- Infection: Your baby will be on antibiotics at birth and for several days after surgery. The surgeon and staff will monitor your baby very closely for any signs of infection.
- Breathing Problems
- Sometimes babies need a blood transfusion. The surgeons will not give blood unless it is medically needed.
- Feeding problems after surgery: It takes several weeks for the intestines to heal properly and can be slow to tolerate food.
Discharge Planning
You will be able to take your baby home once he or she is taking enough formula or breast milk to grow and gain weight. The total length of time your baby will stay in the hospital will vary. It will depend on whether your baby is born with other health issues. The average length of hospital stay is 6 to 8 weeks. A few babies will do especially well and go home earlier.
Looking Ahead
Your baby will need regular follow-up appointments to measure growth, development, and nutrition. You will want to find a local pediatrician to take care of routine checkups, immunizations, and doctor’s visits. The program coordinator can help you if needed. The pediatric surgeon will follow up with your baby’s surgical needs for as long as necessary.